This case report presents an iatrogenic induced mediastinal emphysema after restorative treatment of the lower left second molar, aimed to highlight the potential life-threatening consequences, and providing diagnostics and treatment concepts of complicated dental induced emphysema based on literature review. A 74-year-old female patient was admitted to the emergency department due to a fall on her shoulder. Additional finding was a significant swelling of the face and neck. In the computer tomography of the head, neck, and thorax, a humerus fracture and pronounced soft tissue emphysema from the infraorbital region to the mediastinum was detected. The patient reported that she had been treated by her dentist 4 days earlier. The treatment had to be discontinued after beginning of a pronounced swelling. Other reasons for the emphysema could be excluded out on an interdisciplinary teamwork. The patient was monitored as an inpatient for 5 days and received intravenous antibiotic therapy. This case report shows the rare complication of pronounced mediastinal emphysema after root canal treatment. Emphysema should always be a differential diagnosis of soft tissue swelling and, in case of doubt, a general medical presentation should be made.
Hinweise
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Introduction
Mediastinal emphysema, also called pneumomediastinum, can be spontaneous as well as secondary and is the pathologic presence of free air enclosing mediastinal structures. The secondary mediastinal emphysema is associated with trauma and iatrogenic injury, which can occur after a dental treatment [1]. Emphysema as a complication of dental treatment is a rare complication that is often underestimated. It can occur in various treatments such as root canal treatment, professional teeth cleaning, tooth extraction, conservative, and prosthetic therapy [2‐4]. Although iatrogenic emphysema is a very important differential diagnosis of facial and mediastinal swelling, it is rarely diagnosed by professional dentists and often played down. Whereby the spread of emphysema into the mediastinum can lead to life-threatening consequences, accurate diagnosis of emphysema must be made by clinical and radiological examination [2, 5]. There are several articles in the literature that address the causes of emphysema by dental treatment. This case report describes a pronounced mediastinal emphysema due to tooth preservation treatment in the molar region of the lower jaw, affecting the entire thoracic region and highlighted similar case reports based on literature search performed between 2010 and 2021, regarding their development, extent of disease, diagnostics, and treatment concepts.
Case presentation
A 74-year-old female patient was admitted by an ambulance to the interdisciplinary emergency department of the University Hospital Schleswig–Holstein, Campus Kiel, after a fall on the right shoulder and on the face while walking with her dog. Anamnestically, the patient reported pain in the region of the right shoulder and the right hemithorax. In addition, there was a pronounced swelling of the face and neck, but this had already existed since dental treatment 4 days earlier. The treatment was discontinued after beginning of the swelling. After that, the patient was seen by her general practitioner. According to her medical history, she was given cortisone. Furthermore, the patient reported a hoarse voice immediately after dental practice, which was significantly regressive.
Anzeige
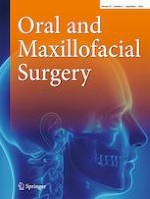
The initial computer tomography of the head and neck revealed prominent left cervical soft tissue emphysema. The emphysema extended to the prevertebral fat lamella and cranially into the Masseter’s lodge (Fig. 1). No fistula was demarcated from the oesophageal or tracheal regions. Furthermore, there was a questionable acute non-displaced fracture of the left nasal bone. There were no acute intracranial or cervical trauma consequences following her fall.
Fig. 1
The spread of emphysema extends from the midface through the masseter loge to the mandibular rim. This was the initial computer tomography from the head until the neck. The emphysema was a secondary diagnosis
×
An X-ray examination (conventional X-ray and computer tomography) of the right shoulder showed a dislocated fracture of the right humeral head. Conventional X-ray examination of the right elbow, the right ribs, and thorax showed no fractures. Additionally, soft tissue emphysema extending from the cervical to the thorax with mediastinal emphysema was detected. A following computer tomography of the thorax (Fig. 2) could not definite a cause for the mediastinal emphysema. Only a slightly dislocated fracture of the 6th and 7th rib on the left ventral side could be detected. In addition, there was a small pleural effusion on the right side and a sintering of the thoracic spine, which appeared to be older.
Fig. 2
Following computed tomography of the thorax was able to diagnose further spread of emphysema. It extended from the neck to retrosternal and into the mediastinum
×
To protect the shoulder fracture, a Gilchrist bandage was applied by the surgical trauma team. A further surgical treatment under general anaesthesia was planned in a few days.
Due to the pronounced emphysema, an oesophageal perforation was excluded by gastroscopy and a bronchoscopy was performed to exclude a cause in the tracheal and pulmonary region.
Anzeige
A clinical presentation to the department of otolaryngology did not reveal a focus on their specialty. The fracture of the nasal bone did not require further treatment. Clinically, only a small abrasion on the nasal bridge was evident.
Thus, the patient was monitored at the Clinic for Oral and Maxillofacial Surgery. The anamnesis and the clinical and radiological examination revealed that the cause of the pronounced soft tissue emphysema was a root canal treatment and restorative treatment of tooth 37 4 days earlier in a dental practice, during which air was insufflated into the surrounding tissue. The treatment started without any problems; immediately after air insufflation, swelling began to spread throughout the infraorbital region. The patient reported that previous dental procedures were performed without pathological abnormalities. The oral inspection revealed no wound or laceration.
On arrival, the patient showed no dyspnoea or respiratory distress. The vital signs showed no danger to life, blood pressure was 140/87 mm Hg, heart rate was 80 beats per minute, respiratory rate was 12 per minute, temperature was 36.6 °C, oxygen saturation was 99%, and Glasgow Coma Scale was 15. On clinical examination, the entire area of swelling appeared soft with noticeable crepitation; however, pain was denied. There was no severe redness, hyperthermia of the tissue, or other pathologic abnormalities. The patient reported taking only aspirin for routine treatment and to be healthy.
Laboratory control showed elevated leukocytes at 12.78 × 10^9/l and C-reactive protein at 85.5 mg/l. The patient was treated as an inpatient and monitored. The patient received intravenous antibiotic therapy with sulbactam/ampicillin 1.5 g three times daily and pain medication as needed. In the laboratory controls, the infection parameters showed regression, and the swelling also showed clinical improvement. Vital signs were without pathological abnormalities at all times. The patient could be discharged home after 5 days in a cardiac and pulmonary good general condition with oral antibiotics. In a follow-up examination 7 days later, the clinical examination showed no further pathological abnormalities.
Literature review
A detailed review of the English literature from 2010 to 2021 was performed using the Pubmed database. The terms “dental”, “dental treatment”, “mediastinal emphysema”, “pneumomediastinum”, and “complications” were used for this purpose. Thirty-three articles could be found and evaluated and are summarised in Table 1. All patients presented a pronounced emphysema from the facial to the mediastinum.
Table 1
A comprehensive review of the literature from 2010 to 2021 was conducted through the PubMed database, using the research terms “dental”, “dental treatment”, “mediastinal emphysema”, “pneumomediastinum”, and “complications”. Developments of emphysema after different dental treatments are shown”
Hospitalisation for five days, diphenhydramine intravenous, flexible laryngoscopy, ampi-cillin/sulbactam, and clindamycin intravenous; intubation, mediastinal drainage one day later because of deterioration of the symptoms. Amoxicillin oral for six days as outpatient
Hospitalisation, mediastinal drainage, intravenous antibiotic: piperacillin/tazobactam, vancomycin, and clindamycin. Moxifloxacin oral for seven days as outpatient
Hospitalisation, intravenous antibiotic: clindamycin, dexamethasone, acidophilus capsules for 24 h; esophagogram because of deterioration of the symptoms; ampicillin and metronidazole intravenous. Amoxicillin/clavulanic acid oral for four days as outpatient
Hospitalisation three days, intravenous antibiotics
In 21 patients (63.6%), the dentists treated only the teeth of the lower jaw. In most cases, the molars were treated (76%). In 48.5%, teeth were extracted; in 51.5%, other dental treatments such as filling therapies, endodontic treatment, and crown preparation were done. Pneumomediastinum was detected with computer tomography of the thorax in 30 patients (90.9%). In five cases (15.2%), further examinations such as gastroscopy and bronchoscopy were performed. The treatment with antibiotics was heterogenous; however, 27 patients got an intravenous antibiotic therapy (81.8%). One patient was treated surgically.
In all cases, the patients evolved well with resolution of the mediastinal emphysema.
Discussion
Emphysema—especially subcutaneous emphysema extending into the mediastinum—are rare complications following dental treatment but can lead to prolonged hospitalisation. Usually, patients have a good prognosis, and within a week, the symptoms should be significantly regressed. However, in rare cases, further surgical intervention, such as a tracheotomy to secure the airway or mediastinal drainage, is necessary [6]. Furthermore, this complication can lead to acute danger to life especially the airway is impaired and even intubation becomes necessary [7]. That is the reason why the patients’ vital parameters were monitored during the hospital stay. The patient and the attending physicians appeared to underestimate the potential danger of mediastinal emphysema previously. Nozewski et al. reported that the actual number of cases detected worldwide would be greatly underestimated and that there is a lack of knowledge about the complication after dental intervention [8].
Anzeige
Other life-threatening complications could be a pneumothorax, an infection as well as a mediastinitis, nerve damage, or cardiac problems [9, 10]. Moreover, in 20 to 30%, a patient has a foramen ovale, and embolism—which can result in neurotoxic effects—can occur as a life-threatening complication. Due to resorption of the emphysema into the cardiovascular system, the air could be immediately transmitted intracranially via the foramen ovale [11, 12]. Therefore, it seems to be necessary to treat patients with pronounced emphysema as inpatients and to ensure that the emphysema is sufficiently diminishing. Concerning this matter, antibiotic therapy should always be considered to avoid superinfection or even sepsis. Further studies recommend prophylactic antibiotic therapy with penicillin until the air has been absorbed naturally [13‐15]. Due to hospital standards, the patient received a broad-spectrum antibiotic (ampicillin/sulbactam) intravenously during her inpatient stay and until the infect parameters were normal. This therapy was continued orally on an outpatient basis and stopped at the aftercare check-up 5 days later because the clinical examination was unobtrusive. Penicillin as a broad-spectrum antibiotic is reported in the literature as an adequate coverage of the buccal flora [11, 13].
During dental procedures, the use of high-speed drills as well as isolation with air nozzles is standard. Nowadays, iatrogenic subcutaneous emphysema in the face can be associated with these treatment steps even during minor dental procedures [16]. As soon as air has entered the soft tissue space, it can spread along the complex fascial planes and anatomic spaces of the face and neck into the mediastinum or retropharyngeal region. In this context, most of the iatrogenic emphysema is described by root canal treatments or tooth extractions in the mandibular and molar region, because of the anatomical connection to these spaces [17‐19]. In addition, preparations and filling therapies of mandibular molar regions can also lead to these complications [20]. Although soft tissue emphysema is more likely as a result from treatments of mandibular teeth due to their anatomical relationships, nevertheless, emphysema can occur also during all dental treatments in the upper jaw by using air supply [21].
In the literature are some studies describing apical inflammations of the second molars of the lower jaw which can lead to unusual abscesses. The spread of inflammation is explained by the lingual root, which can sometimes extend into the mouth base. This provides connections to the cervical fascia and their lodges [22, 23]. In the coronal slice of the computed tomography scan, the lingual root of tooth 37 can also be seen (Fig. 3). The root extends far lingually into the mouth base. Thus, during insufflation of root canal treatment, air will have entered the cervical fascia and cervical lodges. In the majority of the papers, recruited removal of the second and third molar teeth seems to be the main reason for mediastinal emphysema development in the dental practice.
Fig. 3
The lingual root canal of the lower left molar lays into the mouth base. The yellow arrow highlighted the entrance of the air into the cervical fascia and their lodges
×
The subcutaneous emphysema may occur within minutes to hours after dental surgery. Erroneously, soft tissue emphysema is often misdiagnosed as an allergic reaction or acute postoperative swelling [24]. Subcutaneous emphysema and mediastinal emphysema usually do not have dental causes. More often are causes as traumatic intubation, mechanical ventilation, facial trauma, violent vomiting with rupture of the oesophagus, asthma exacerbation with alveolar rupture, or surgical procedures in the head and neck region [25]. Although our patient presented to a general practitioner because of the swelling, her medical history was incorrectly treated as a mild allergic reaction and cortisone was administered. A more detailed clinical examination and diagnosis could have ruled out an allergic reaction, especially since no other allergic symptoms such as cardio-respiratory problems occurred in the patient [26]. Angioedema, allergic reactions caused by the local anaesthetic, haematomas, and soft tissue infections are important differential diagnosis. Detailed history, clinical examination including palpable crepitations, and radiologic imaging can usually diagnose emphysema [27]. Figure 4 provides a guideline in the diagnosis of mediastinal emphysema.
Fig. 4
This diagram enables a guideline in medical diagnostics and therapy of the mediastinal emphysema, especially after dental treatments. Initially, a detailed anamnesis should be obtained to identify the probable cause of the mediastinal emphysema. The following clinical examination as well as the X-ray and laboratory diagnostic give an indication of the extent of the disease. If the cause of the mediastinal emphysema is still unclear, further medical examinations should be performed. In case of pronounced symptoms and clinical manifestation of the mediastinal emphysema, inpatient monitoring should be recommended
×
Anzeige
The major limitation of this case report is that the computer tomography was performed on an emergency basis, whereby the representation of the teeth is only imprecise. The exact way of the roots of the second molar can only be estimated. For further diagnosis, a dental computed tomography would be necessary.
Conclusion
This case report of pronounced facial and mediastinal emphysema after tooth preservation of the second molar in the lower jaw demonstrates how quickly an iatrogenic emphysema can be overlooked by treating professional physicians without further diagnosis. Soft tissue emphysema is a rare complication of dental treatment as root canal treatment or filling therapy, but it should always be considered as a differential diagnosis. Particularly soft tissue emphysema, especially those extending into the mediastinum, can present life-threatening complications. Moreover, the review of the literature shows developments of emphysema after different dental treatments, intending, to reduce the lack of knowledge of complications after dental treatments.
Thus, a medical consultation should always be made and the need for inpatient monitoring should be discussed. At least, the prescription of a prophylactic broad-spectrum antibiotic should be considered.
Declarations
Competing interests
The authors declare no competing interests.
Anzeige
Ethics approval
Ethical approval was obtained from the Ethic Commission of the Faculty of Medicine at the Christian-Albrechts-University, Kiel (D463/22). The patient provided informed consent.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
The authors affirm that human research participants provided informed consent for publication.
Conflict of interest
The authors declare no competing interests.
Open AccessThis article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
In der Notaufnahme wird die Chance, Opfer von häuslicher Gewalt zu identifizieren, von Orthopäden und Orthopädinnen offenbar zu wenig genutzt. Darauf deuten die Ergebnisse einer Fragebogenstudie an der Sahlgrenska-Universität in Schweden hin.
Darüber reden und aus Fehlern lernen, sollte das Motto in der Medizin lauten. Und zwar nicht nur im Sinne der Patientensicherheit. Eine negative Fehlerkultur kann auch die Behandelnden ernsthaft krank machen, warnt Prof. Dr. Reinhard Strametz. Ein Plädoyer und ein Leitfaden für den offenen Umgang mit kritischen Ereignissen in Medizin und Pflege.
Ein Frauenanteil von mindestens einem Drittel im ärztlichen Op.-Team war in einer großen retrospektiven Studie aus Kanada mit einer signifikanten Reduktion der postoperativen Morbidität assoziiert.
Bei schwerer Aortenstenose und obstruktiver KHK empfehlen die Leitlinien derzeit eine chirurgische Kombi-Behandlung aus Klappenersatz plus Bypass-OP. Diese Empfehlung wird allerdings jetzt durch eine aktuelle Studie infrage gestellt – mit überraschender Deutlichkeit.
Update Chirurgie
Bestellen Sie unseren Fach-Newsletterund bleiben Sie gut informiert.
Das Karpaltunnelsyndrom ist die häufigste Kompressionsneuropathie peripherer Nerven. Obwohl die Anamnese mit dem nächtlichen Einschlafen der Hand (Brachialgia parästhetica nocturna) sehr typisch ist, ist eine klinisch-neurologische Untersuchung und Elektroneurografie in manchen Fällen auch eine Neurosonografie erforderlich. Im Anfangsstadium sind konservative Maßnahmen (Handgelenksschiene, Ergotherapie) empfehlenswert. Bei nicht Ansprechen der konservativen Therapie oder Auftreten von neurologischen Ausfällen ist eine Dekompression des N. medianus am Karpaltunnel indiziert.
Das Webinar beschäftigt sich mit Fragen und Antworten zu Diagnostik und Klassifikation sowie Möglichkeiten des Ausschlusses von Zusatzverletzungen. Die Referenten erläutern, welche Frakturen konservativ behandelt werden können und wie. Das Webinar beantwortet die Frage nach aktuellen operativen Therapiekonzepten: Welcher Zugang, welches Osteosynthesematerial? Auf was muss bei der Nachbehandlung der distalen Radiusfraktur geachtet werden?
Inhalte des Webinars zur S1-Leitlinie „Empfehlungen zur Therapie der akuten Appendizitis bei Erwachsenen“ sind die Darstellung des Projektes und des Erstellungswegs zur S1-Leitlinie, die Erläuterung der klinischen Relevanz der Klassifikation EAES 2015, die wissenschaftliche Begründung der wichtigsten Empfehlungen und die Darstellung stadiengerechter Therapieoptionen.