This retrospective study aims to define the optimal timing of the surgical treatment of orbital floor trapdoor fractures (OFTFs) in adults according to clinical and radiological findings.
Methods
From January 2006 to December 2020, 382 patients with isolated orbital floor fracture were admitted to the Division of Maxillofacial Surgery of Turin, Italy. The criteria for inclusion were age ≥ 16 years, preoperative computed tomography showing a linear (1a) or medial hinge fracture (1b), diplopia, and 6 months of follow-up data. Aetiology and mechanism of injury, presence of post-traumatic enophthalmos and oculocardiac reflex, time between trauma occurrence and surgery [stratified as < 24 h (urgent treatment), 24–96 h (early treatment), and > 96 h (late treatment)], days of hospitalisation, and clinical outcomes were examinated.
Results
Twenty-four patients (18 males; mean age, 23.2 years) presented with OFTFs. The most common cause was sport injury (50%). Type 1a fracture was observed in eight patients (mean age, 19.5 years), type 1b fracture in 16 patients (mean age, 23.6 years). Urgent, early, and late treatments were performed in eight patients each. The mean time between trauma occurrence and surgery was 3,8 days (range: 0–17 days). Resolution of diplopia was observed 1 week after surgery in 10 patients, 1 month in 12. Diplopia persisted in 2 patient, both treated > 96 h after trauma.
Conclusion
Although the number of patients was too small to define a standard protocol, the authors recommend early treatment of adult OFTFs to promote complete resolution of diplopia.
Hinweise
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Introduction
First described in 1965 by Soll and Poley [1], orbital floor trapdoor fractures (OFTFs) are commonly considered primary emergencies in paediatric maxillofacial traumatology, as well as a clinical variant described in 1998 by Jordan et al., defined “white eyed blowout” due to little clinical evidence of periorbital trauma [2].
Several authors have stated that in patients with vertical eye movement restricted caused by entrapment of the inferior rectus muscle or peri-muscular connective tissue, surgical treatment of OFTFs should be performed as soon as possible to reduce the risk of permanent diplopia [2‐7]. However, there is no universal consensus regarding the indications and timing of surgical treatment for rare OFTFs in adults, as indicated by various case reports [8‐16], and case series (typically involving few patients) [17‐21].
Anzeige
Therefore, the purpose of this retrospective analysis was to define the indications and evaluate the optimal timing of the surgical treatment of OFTFs in adults, according to clinical findings and radiological fracture types. Accordingly, we analysed the long-term results of adult patients who underwent surgery for treatment of OFTFs in our hospital during the past 15 years.
Methods
From January 2006 to December 2020, 2274 patients with maxillofacial fractures were admitted to the Division of Maxillofacial Surgery, Città della Salute e della Scienza Hospital, University of Turin (Turin, Italy); 382 of these patients exhibited isolated orbital floor fracture. The criteria for inclusion in the present retrospective study were as follows: age ≥ 16 years, availability of preoperative computed tomography scans with coronal view of the orbit, clinical evidence of diplopia and restricted eye movement, and at least 6 months of follow-up data.
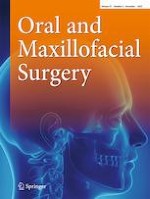
All the orbital floor fractures were radiologically classified according to Gerbino et al. [22] (Fig. 1) in type 1a, when a fracture line running along the infraorbital nerve canal to the retrobulbar area, with bone displacement smaller than the orbital floor thickness, and type 1b when a small medial part of the orbital floor was displaced downward further than the orbital floor thickness, along with a medial hinge.
Fig. 1
Preoperative CT scan, coronal view: a OFTF type 1a or linear fracture; b OFTF type 1b or hinged fractures according to Gerbino et al.
×
Patients with incomplete clinical and radiological records, as well as those who had not completed postoperative follow-up examinations, were excluded from the study. The following data were examined in this study: trauma aetiology and mechanism, clinical evidence of post-traumatic enophthalmos, clinical signs of oculocardiac reflex, time between trauma occurrence and surgery [stratified as < 24 h (urgent treatment), 24–96 h (early treatment), and > 96 h (late treatment)] [2], days of hospitalisation, and clinical outcomes.
Anzeige
All surgical treatments were performed under general anaesthesia; administration of high-dose steroids was initiated before surgery and continued for 72 h postoperatively. Surgical repairs were performed using the subciliary or transconjunctival approach to expose the orbital floor. After each fracture had been visualised, the herniated tissue was gently dissected and reduced into the orbit. In all patients, Lyoplant (Braun, Tuttlingen, Germany) was placed on the orbital floor to cover the bone defect. At the end of each intervention, a duction test was performed. Patients were advised to return to the clinic for follow-up examinations, weekly for the first month after surgery and then monthly for 6 months. During follow-up visits, diplopia and ocular motility were recorded using the Hess–Lancaster screen.
Results
Among 382 patients with pure orbital floor fractures, 24 (6.3%; 18 males and 6 females; mean age, 23.2 years (range: 16–47 years)] presented with OFTFs. OFTFs were caused by sports injuries in 12 patients, assault in 11 patients, and a fall in 1 patient (Table 1). The main mechanism of injury was a punch during a violent incident or collision with against another player during a sporting event (Table 2).
Table 1
Adult patients who underwent surgery for OFTF between 2006 and 2020
No
Age (yr)
Gender
Cause
Type of fracture
Interval to surgery (h)
1
16
M
Sport
1b
24–96
2
16
M
Violence
1a
< 24
3
17
M
Sport
1a
< 24
4
17
M
Violence
1b
< 24
5
17
M
Violence
1a
< 24
6
17
M
Sport
1b
24–96
7
18
M
Violence
1b
24–96
8
18
M
Fall
1b
24–96
9
18
F
Sport
1b
< 24
10
19
M
Sport
1a
> 96
11
20
M
Violence
1a
24–96
12
21
M
Violence
1b
< 24
13
21
M
Sport
1a
> 96
14
22
F
Violence
1b
> 96
15
22
M
Sport
1a
24–96
16
23
M
Sport
1b
24–96
17
24
M
Violence
1a
< 24
18
29
M
Violence
1b
< 24
19
29
M
Sport
1b
> 96
20
30
F
Sport
1b
24–96
21
30
F
Sport
1b
> 96
22
31
F
Violence
1b
> 96
23
34
F
Violence
1b
> 96
24
47
M
Sport
1b
> 96
F female, M male, h hour, yr years
Table 2
Type of OFTF in relation to the mechanism of maxillofacial trauma
Type Ia
Type Ib
Total
Violence
Fist
4
6
10
Kick
0
1
1
Sport
Other player
3
5
8
Ground
1
2
3
Object
0
1
1
Other
Ground
0
1
1
Type 1a fracture was observed in eight patients (mean age, 19.5 years), while Type 1b was observed in 16 patients (mean age, 23.6 years). Table 2 summarises the distribution of fracture types by injury mechanism. No patients older than 24 years exhibited type 1a OFTFs, and none exhibited post-traumatic enophthalmos or signs of oculocardiac reflex.
Surgery was performed as soon as possible, i.e. within 12 h of presentation; thus, the time between the occurrence of the trauma and surgery was influenced by the timing of presentation. Urgent, early, and late treatments were performed in eight patients each. The mean time between trauma occurrence and surgery was 3.8 days (range: 0–17 days), and the mean hospital stay was 3 days.
At the follow-up examination, resolution of diplopia was observed 1 week after surgery in 10 patients (5 had undergone surgery within 24 h of trauma, 1 within 24–96 h, and 4 > 96 h). Resolution of diplopia was observed at the 1-month follow-up examination in 12 of the remaining 14 patients (3 had undergone surgery within 24 h of trauma, 7 within 24–96 h, and 2 > 96 h). In the final two patients, diplopia persisted only in the upper field of gaze. Table 3 summarises the relationships among fracture type, timing, and outcomes.
Table 3
Relationship among time of surgery, type of OFTF, and outcome (resolution of diplopia)
Time of surgery (h)
Type of fracture
No. of patients
1 week
1 month
Not solved after 6 months
< 24
1a
4
2
2
0
1b
4
3
1
0
24–96
1a
2
1
1
0
1b
6
0
6
0
≥ 96
1a
2
2
0
0
1b
6
2
2
2
Total
24
10
12
2
Discussion
Progressive loss of elasticity of bone tissues in adults, particularly involving the orbital floor, causes the bone to become more susceptible to displaced or comminuted fractures, and is often associated with other facial fractures [2, 7, 18, 20]. Therefore, pure fractures (i.e. with minimal displacement of the orbital floor or entrapment of the orbital soft tissues) are rare among adults, especially compared with the paediatric population [4, 7, 19, 21], in which the orbital wall is likely to bend, crack, and then to return to its normal position causing the orbital content to be trapped into the fracture [2, 9].
In this retrospective analysis of all pure orbital floor fractures surgically treated in our hospital, OFTFs were present in 6.3% of patients; this was similar to the rate reported by Takahashi et al. [7]. This rare type of fracture mainly affects young adult males and boys in the second decade of life, according to published case reports [8‐16], and case series [17‐21], involving patients over 30 years of age (Table 4). The most frequent aetiologies of this type of orbital fracture in our study were similar to the literature (i.e., assault and sports injuries). In addition, consistent with numerous reports [11, 13, 17, 18], the trauma aetiology generally did not involve road traffic accidents [15, 18, 20], or falls [8], which represent the main causes of maxillofacial fractures. In this study, direct trauma to the orbital region results from a medium- or low-speed impact (generally following an assault or collision with an opponent during a sporting event), which produce twofold more type 1b than type 1a fractures. Furthermore, type 1b fractures increase in frequency with age, such that no 1a fractures have been reported in patients older than 24 years of age [21]. Notably, oculocardiac reflex and enophthalmos were not encountered in our sample population; these manifestations are very rare in adults.
Table 4
Summary of adult OFTF published in the recent literature
Gender
Age
Cause
Presentation
Time of surgery (days)
Outcome
Sires et al. (1998)
M
20
Fall
Diplopia, OR
3
Diplopia
Kakizaki et al. (2005)
M
20
Blunt trauma (elbow)
Diplopia, OR
16
Diplopia sup
Kum et al. (2009)
M
37
Work
Diplopia
21
Diplopia sup
Mehanna et al. (2009)
M
17
Assault
Diplopia, OR
24
No diplopia
M
21
Assault
Diplopia, OR
6
Diplopia
Yano et al. (2010)
M
16
Assault
Diplopia
5
No diplopia
M
17
Sport
Diplopia
12
ND
M
18
Sport
Diplopia
8
ND
M
24
Sport
Diplopia
10
ND
Ethunandan and Evans. (2011)
M
16
RTA
Diplopia, OR
3
Diplopia sup
F
16
Sport
Diplopia, OR
7
No diplopia
F
17
Assault
Diplopia
11
Diplopia sup
M
21
Assault
Diplopia, OR
< 1
No diplopia
M
29
Sport
Diplopia
17
Diplopia sup
F
53
Assault
Diplopia, OR
41
No diplopia
Summers et al. (2017)
M
26
Assault
Diplopia
ND
ND
Papadiochos et al. (2019)
M
29
Assault
Diplopia, OR
5
No diplopia
Said et al. (2019)
M
23
ND
Diplopia
ND
ND
Karthik et al. (2019)
M
16
Assault
Diplopia
11
Diplopia sup
M
17
Assault
Diplopia
> 1
No diplopia
M
24
Assault
Diplopia
6
Diplopia sup
F
27
RTA
Diplopia
48
No diplopia
M
29
RTA
Diplopia
< 1
No diplopia
Brasileiro et al. (2020)
F
26
RTA
Diplopia, OR
1
No diplopia
Gowda et al. (2020)
F
25
ND
Diplopia
3
Diplopia sup
Al-Qattan et al. (2021)
M
25–50
ND
Diplopia
< 2
No diplopia
F female, M male, ND not defined, OR oculocardiac reflex, RTA road traffic accident
Although Scolozzi et al. [23] reported that guidelines in several centres continue to include a waiting period of 14 days before surgery in patients with blowout fractures who exhibit persistent diplopia in primary gaze with restricted ocular motility, there remains a general consensus supporting urgent surgical treatment of OFTFs in both adult and paediatric patients [2‐7]. In a series of 10 adult trapdoor fractures (including 7 pure), all surgically treated within 48 h, Al-Qattan and Al-Qattan did not encounter postoperative diplopia [21]. Similarly, no cases of diplopia were reported by Mehanna et al. [11] or Brasileiro et al. [15], among patients who had undergone surgery within 24 h. Karthik et al. [20] observed that among four adult cases of OFTF, the two patients who experienced the greatest delays between trauma and surgery (8 and 9 days, respectively) exhibited the worst outcomes; Ethunandan et al. [18]reported similar outcomes in 2 patients surgically treated at 11 and 17 days after trauma. Takahashi et al. [7] suggested that a long interval between trauma and surgery could promote fibrotic and necrotic changes in entrapped tissues, causing greater postoperative restriction of ocular mobility. In contrast, Kwon et al. [4] suggested that OFTFs with severe muscle limitations should be surgically treated in adult patients within 5 days after trauma; in a recent review of the literature, Papadiochos et al. [13] observed that non-emergent OFTFs in adults showed satisfactory outcomes even when treatment was delayed beyond the 48 or 72 h recommended for paediatric patients. Various studies [7, 13, 17, 24, 25] have suggested that the difference in surgical timing between adults and children could be explained by the better prognosis for type 1b OFTFs, which are more common in adults; the larger amount of trapped tissue in children (i.e. inferior rectus muscle within the fracture gap), rather than the considerable differences in necrosis and fibrosis, makes treatment more urgent in these patients.
Anzeige
Although the low number of OFTFs in this study may have obscured statistically significant differences in the prognoses of patients with type 1a versus 1b fractures, analysis of treatment timing showed that only two patients (both surgically treated > 96 h after trauma) did not exhibit diplopia resolution at the 6-month follow-up examination. In our hospital, the treatment timing for paediatric and adult patients with OFTFs is similar; thus, patients aged over 15 years undergo surgery as soon as possible. This early surgery can easily (and often non-traumatically) release the muscle and/or entrapped orbital tissues.
Conclusion
This retrospective study showed that pure OFTFs in adults almost exclusively affected young boys and males under 30 years of age; moreover, they were caused by low-to-medium energy impacts (almost exclusively sports injuries or violent assaults) and type 1b fractures were more common with advancing age. Finally, although the number of patients was too small to define a standard treatment protocol, the authors recommend early treatment of this rare type of orbital fracture, because urgent and early treatments can achieve complete resolution of diplopia.
Declarations
Ethical approval
This is an observational study. The Research Ethics Committee of University of Study of Torino has confirmed that no ethical approval is required.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Anzeige
Consent for publication
The authors affirm that human research participants provided informed consent for publication of the images in Fig. 1a and b.
Competing interests
The authors declare no competing interests.
Open AccessThis article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
In der Notaufnahme wird die Chance, Opfer von häuslicher Gewalt zu identifizieren, von Orthopäden und Orthopädinnen offenbar zu wenig genutzt. Darauf deuten die Ergebnisse einer Fragebogenstudie an der Sahlgrenska-Universität in Schweden hin.
Darüber reden und aus Fehlern lernen, sollte das Motto in der Medizin lauten. Und zwar nicht nur im Sinne der Patientensicherheit. Eine negative Fehlerkultur kann auch die Behandelnden ernsthaft krank machen, warnt Prof. Dr. Reinhard Strametz. Ein Plädoyer und ein Leitfaden für den offenen Umgang mit kritischen Ereignissen in Medizin und Pflege.
Ein Frauenanteil von mindestens einem Drittel im ärztlichen Op.-Team war in einer großen retrospektiven Studie aus Kanada mit einer signifikanten Reduktion der postoperativen Morbidität assoziiert.
Bei schwerer Aortenstenose und obstruktiver KHK empfehlen die Leitlinien derzeit eine chirurgische Kombi-Behandlung aus Klappenersatz plus Bypass-OP. Diese Empfehlung wird allerdings jetzt durch eine aktuelle Studie infrage gestellt – mit überraschender Deutlichkeit.
Update Chirurgie
Bestellen Sie unseren Fach-Newsletterund bleiben Sie gut informiert.
Das Karpaltunnelsyndrom ist die häufigste Kompressionsneuropathie peripherer Nerven. Obwohl die Anamnese mit dem nächtlichen Einschlafen der Hand (Brachialgia parästhetica nocturna) sehr typisch ist, ist eine klinisch-neurologische Untersuchung und Elektroneurografie in manchen Fällen auch eine Neurosonografie erforderlich. Im Anfangsstadium sind konservative Maßnahmen (Handgelenksschiene, Ergotherapie) empfehlenswert. Bei nicht Ansprechen der konservativen Therapie oder Auftreten von neurologischen Ausfällen ist eine Dekompression des N. medianus am Karpaltunnel indiziert.
Das Webinar beschäftigt sich mit Fragen und Antworten zu Diagnostik und Klassifikation sowie Möglichkeiten des Ausschlusses von Zusatzverletzungen. Die Referenten erläutern, welche Frakturen konservativ behandelt werden können und wie. Das Webinar beantwortet die Frage nach aktuellen operativen Therapiekonzepten: Welcher Zugang, welches Osteosynthesematerial? Auf was muss bei der Nachbehandlung der distalen Radiusfraktur geachtet werden?
Inhalte des Webinars zur S1-Leitlinie „Empfehlungen zur Therapie der akuten Appendizitis bei Erwachsenen“ sind die Darstellung des Projektes und des Erstellungswegs zur S1-Leitlinie, die Erläuterung der klinischen Relevanz der Klassifikation EAES 2015, die wissenschaftliche Begründung der wichtigsten Empfehlungen und die Darstellung stadiengerechter Therapieoptionen.